Study Paper prepared by: Balram Jo
ABSTRACTStatus of Nutrition has been hit hard by the Pandemic caused by COVID 19 all over the world, challenging the already existing service delivery system, health care and governance to address the collateral damages caused by this Pandemic. Numerous statistical data and researches have provided the overview of the nutritional status of India at large and also the state wise data on nutrition and its components prior to this Pandemic. One can assume the damages pandemic has added to already existing lot of Nutritional Challenges in the Country and specifically in the state of Jharkhand.
This Paper focuses on the four such government schemes such as ICDS (Integrated Child Development Scheme), MDM (Mid-day meal), PDS (Public Distribution Scheme) and Maternity schemes and the impact of Pandemic on the implementation of these schemes and on the community in the various pocket of Jharkhand. Prevalence of large number of people without Ration card and access to food has heightened Malnutrition in Jharkhand making large section of people slip into Extreme Hunger Group. In spite of existing challenges some good Practices introduced by CSOs in the state and in the neighbouring state are excellent in addressing the issue of Malnutrition which can be implemented in the state of Jharkhand. Recommendations on strategies to combat Malnutrition are also highlighted in this Paper.
INTRODUCTIONNutrition is vital for the overall wellbeing of a Person. Start from the conceiving of foetus in the womb Nutrition is fundamental in building up of foetus with time. Deficiency in nutrition component have a lifelong impact on the physical, Psychological and social wellbeing of a person. As per the Global Nutrition Report of 2020 India is among many other countries which might miss the global nutrition Target 2025. As per the report of NFHS 4 Malnutrition in Jharkhand is alarming and it Ranks 1st Stunting, anaemia in Pregnancy, and Underweight leaving behind Bihar and Madhya Pradesh and 2nd in wasting, Anaemia in Children preceded by Bihar and followed by Meghalaya. As per the Census 2011, Population of Jharkhand is 3.3 Crore with 24.05% urban population.
Many policies and schemes has been developed by the Govt.of India to address the Problem of Malnutrition in the Country among which ICDS( Integrated Child Development Scheme), MDM( Mid-Day Meal), PDS( Public Distribution Scheme) and Maternity benefit schemes will be given a close look in this paper.
Status of Jharkhand in malnutrition through the lens of NFHS3 and NFHS 4 data:Malnutrition is one of the major problems in the country. As per the NFHS 3 and NFHS 4 data, the status of India as a whole and comparative data of the status of Jharkhand, Madhya Pradesh, Kerala and Rajasthan is present in Table 1.
| Particulars | India | Jharkhand | Madhya Pradesh | Rajasthan | Bihar | Kerala | Goa |
|---|---|---|---|---|---|---|---|
| Mothers who had full antenatal care(%) | 21 | 8 | 11.4 | 9.7 | 3.3 | 61.2 | 63.4 |
| Children age 12-23 months fully immunized (BCG, measles, and 3 doses each of polio and DPT) (%) | 62 | 61.9 | 53.6 | 54.8 | 61.7 | 82.1 | 88.4 |
| Children under age 3 years breastfed within one hour of birth (%) | 41.6 | 33.1 | 34.4 | 28.4 | 35.9 | 64.3 | 73.3 |
| Children under age 6 months exclusively breastfed (%) | 54.9 | 64.8 | 58.2 | 48.2 | 53.4 | 53.3 | 60.9 |
| Breastfeeding children age 6-23 months receiving an adequate diet (%) | 8.7 | 7.2 | 6.9 | 3.4 | 7.3 | 21.3 | 9.1 |
| Non-breastfeeding children age 6-23 months receiving an adequate diet (%) | 14.3 | 7.1 | 4.9 | 3.7 | 9.2 | 22.3 | 15.1 |
| Total children age 6-23 months receiving an adequate diet (%) | 9.6 | 7.2 | 6.6 | 3.4 | 7.5 | 21.4 | 10.4 |
| Children under 5 years who are stunted (height-for-age) % | 38.4 | 45.3 | 42 | 39.1 | 48.3 | 19.7 | 20.1 |
| Children under 5 years who are wasted (weight-for-height)% | 21 | 29 | 25.8 | 23 | 20.8 | 15.7 | 21.9 |
| Children under 5 years who are severely wasted (weight-for-height) % | 7.5 | 11.4 | 9.2 | 8.6 | 7 | 6.5 | 9.5 |
| Children under 5 years who are underweight (weight-for-age) % | 35.8 | 47.8 | 42.8 | 36.7 | 43.9 | 16.1 | 23.8 |
| Women whose Body Mass Index (BMI) is below normal (BMI < 18.5 kg/m2 ) % | 22.9 | 31.5 | 28.4 | 27 | 30.4 | 9.7 | 14.7 |
| Men whose Body Mass Index (BMI) is below normal (BMI < 18.5 kg/m2 ) % | 20.2 | 23.8 | 28.4 | 22.7 | 25.4 | 8.5 | 10.8 |
| Children age 6-59 months who are anaemic ( < 11.0 g/dl) % | 58.6 | 69.9 | 74 | 60.3 | 63.5 | 35.7 | 48.3 |
| Non-pregnant women age 15-49 years who are anaemic ( < 12.0 g/dl) % | 53.2 | 65.3 | 52.4 | 46.8 | 60.4 | 34.7 | 31.4 |
| Pregnant women age 15-49 years who are anaemic ( < 11.0 g/dl) % | 50.4 | 62.6 | 54.6 | 46.6 | 58.3 | 22.6 | 26.7 |
| All women age 15-49 years who are anaemic (%) | 53.1 | 65.2 | 52.5 | 46.8 | 60.3 | 34.3 | 31.3 |
The following graphical representation of District wise stunting, wasting SAM and Underweight status of Jharkhand.
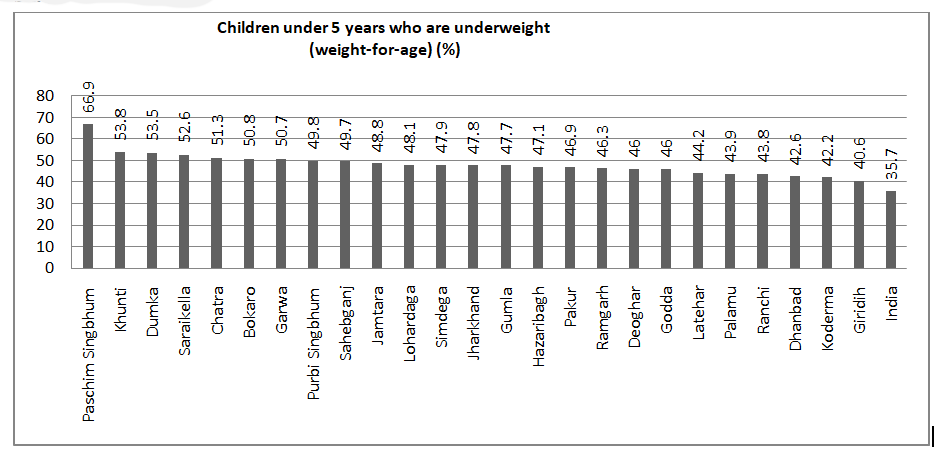
Fig 4: District wise Distribution of children under 5 years who are underweight. (Source NFHS 4)
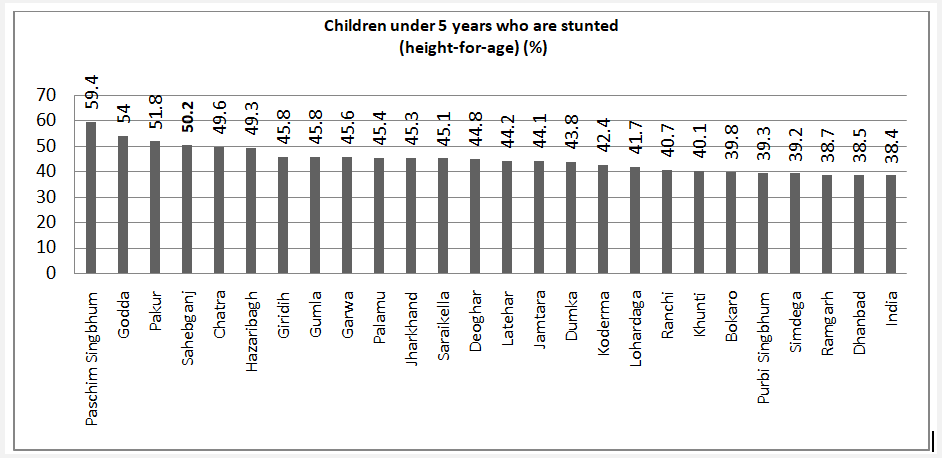
Fig 5: District wise distribution of Children under 5 years who are stunted. (Source NFHS 4)
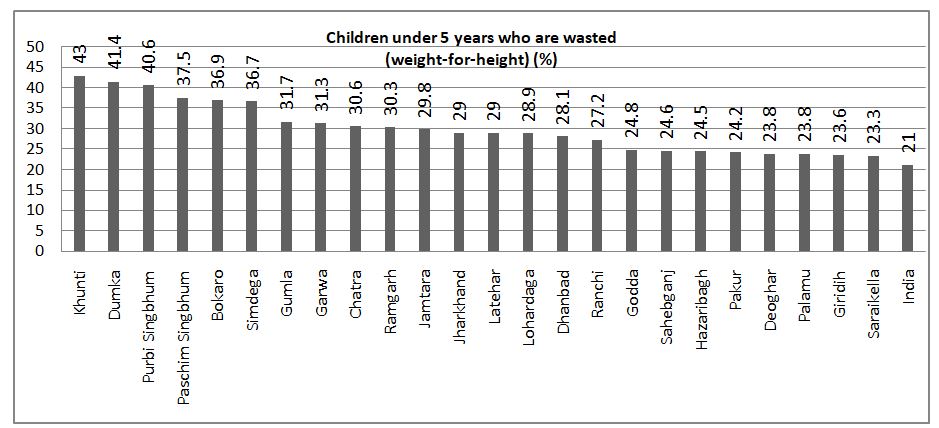
Fig6: District wise distribution of Children under 5 years who are wasted. (Source NFHS 4)
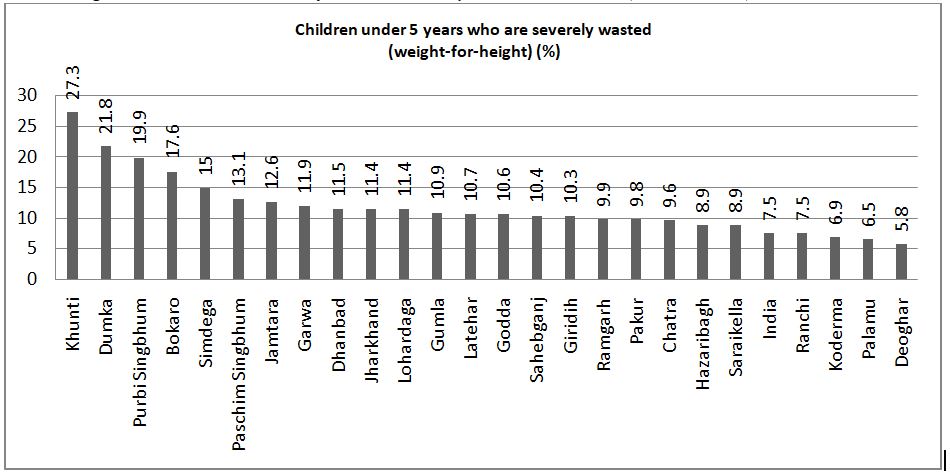
Fig 7: District wise distribution of Children under 5 years who are severely wasted. (Source NFHS 4)
Figure 4,5 6,and 7 Shows that PaschimSingbhum, Khuti and Dumka has the highest percentage of underweight children, PaschimSingbhum, Gooda and Pakur has the highest percentage of stunted children under 5, Khunti, dumka , PurbiSingbhum and PaschimSingbhum has the highest percentage of children under 5 years of age who are severely wasted and Severely wasted.
It is noteworthy to mention here and equally alarming that this Data given above are from the Pre COVID time, before the advent of this on-going Pandemic. It is a known fact that This Pandemic has exposed the fragility of our health care system and made the already vulnerable group more vulnerable to Malnutrition and other health Hazards.
Government of India has formulated numerous schemes to improve the nutritional status of the country by addressing Malnutrition at its core. Among many such schemes which are being implemented throughout the Country, this paper will discuss on 4 major Schemes running in the State of Jharkhand which directly addresses Nutrition.
- ICDS:Integrated Child Development Scheme
Integrated Child Development Scheme was launched in the year 1975 by the Govt.of India, initially with 33 blocks. This Scheme comprises of 6 Services such as Supplementary nutrition, Pre School Education, Nutrition and Health Education, Immunization, Health Check-up and Referral Services for children of age 0-6, Adolescent up to 19 yrs. of age, Pregnant and lactating women and eligible couple (between 14 to 54yrs). This Scheme is implemented through AWC (Aaganwadi Centres). In Rural Area one AWC covers 1000 population whereas in Tribal/ Riverine/Dessert and hilly region one AWC covers 300- 700 populations and Mini AWC covers 150-300 population.
Supplementary Nutrition: ICDS provides supplementary nutrition to children of 6 to 72 months severely undernourished children (6-72 months) and Pregnant and lactating women. Supplementary Nutrition is provided on a daily basis to ensure the intake of calorie and protein, deficiency of which impact largely on Malnutrition. Age appropriate THR (Take home ration) are also provided for the children below 3 years and Pregnant & lactating mothers.
Table below shows the daily nutritional supplements provided in the AWC:AGE GROUP CALORIE (kcl) PROTEIN(g) Children ( 6-72 month) 500 12-15 severely undernourished Children 800 20-25 Pregnant women and lactating mother 600 18-20 Table 2: Distribution of Protein and Calories as per the age groups. (Source: MWCD)
- Mid-Day Meal ( MDM)
In the year 1995 National programme on nutritional support to primary education was centrally launched (NP-NSPE), later in the year 2001MDMS started in the form of cooked meal every day for every children of the government and government aided primary school with 300 calories of energy and 8-12 grams of protein. Again in the following year of 2004 and 2007, this scheme was further improvised making the schemes accessible to children studying from class 6 to 8 in any Government, Government aided Primary school and local body school and the daily nutrition intake was raised to 700 calories and 20gram protein for children of Upper Primary section. As per the report published by Save the Children on Dec 2016, 10 crore children in India were covered under the scheme, and Economic Times dated 22Dec. 2019 stated that 11 crore students across 11.34 lakh school are reached by this scheme. Table below provide the Prescribed Nutritional content of the mid-day meal.
ITEM/ PARTRICULAR PRIMARY ( CLASS I TO V) UPPER PRIMARY ( CLASS V-VIII) Calorie ( kcl) 450 700 Protein (g) 12 20 Table3: Distribution of Calorie and Protein in mid-day meal.
Public Distribution System (PDS): PDS was launched by the govt. of India in the year 1997 to provide some supplementary Nutrition in terms of Food Grains to address the scarcity of food grains among the people below Poverty line and Extreme hunger. This Provision does not cover the overall nutrition requirement of a person but provide supplementary quantity of Nutrition. It is also to be noted that Only Ration Card holder can have access to this schemes. Current provision of Food Grains under this Scheme is 5 Kg food grains per person per month.
- Maternity benefit schemes and Programme: Govt. of India through the Ministry of Women and Child Development has introduced and implemented various benefit schemes and programme for the overall wellbeing of the women. Indira Gandhi MatritvaSahayogYozna and ICDS play a vital role in addressing the financial and nutritional issues during Maternity. Financial support through Cash benefits of Rs.6000 in two instalment are given through account transaction of the beneficiary to support the Health and Nutrition need during this time apart from other services available through these schemes. ICDS through AWC provides 600 Calories and 18-20g Protein.
National Institute of Nutrition has given the details about the nutrition requirement of a person. Table below provides the analysis of quantitative requirements of various nutrients among the pregnant women, Lactating mothers and children.
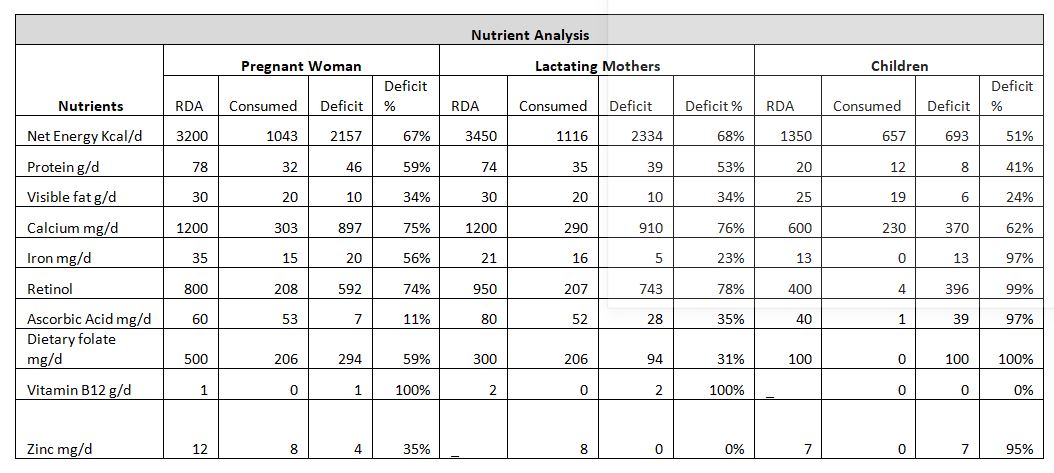
Table 4: Analysis of Nutritinal requirement of Pregnant women, Lactating Mothers and Children.
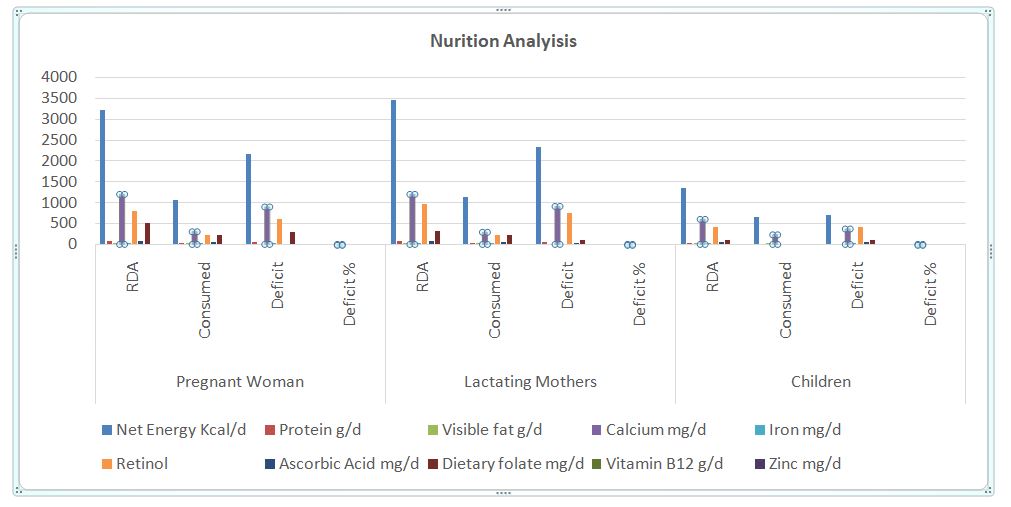
Fig 1: Graphical representation of Nutrition analysis.
As per the study published on May2020 by John Hopkins Blomberg School of Public Health (America), India contributes 20% in Global malnutrition and would exceed 10% more in this Pandemic. This study furthers reflects that the hurdle accessing services will also have a huge effect. It is estimated that 11.57 lakh children and 56700 mothers will lose their lives globally in 6 month. Looking into India’s Health and Nutritional services affected due to COVID will increase the number of maternal and new-born deaths. It is estimated that 49850 more child death and 2398 maternal death will happen. It further claims that due to this pandemic situation services like immunisation, IFA supply, Nutritional services, services for new born care, safe institutional delivery etc were affected very badly and these services were reduced up to 40-50%, therefore India’s share on Malnutrition will increase from 21% to 31.5% globally.
As per the recent study conducted by studies of APU and Sambodhi (27th April- 2nd May) in 47 remote districts of 12 states, the impact of COVID on Hinterland coping shows the vast cascading effect of COVID 19 induced lockdown. It is found that during this lockdown there is a rapid increase in the Drudgery among the women members with 61% more time engaged in fetching water among the returned migrants and 45% among the no returned migrants. It is noteworthy to mention here that this lockdown has induced 77% increase in demand for fuelwood among the returned migrants and 44% among the no returned migrants and also increase in time for collecting fuelwood by 68% among the returned migrants and 47% among the no returned migrants. It is alarming fact that this indicates the rapid increase in deforestation in these 47 remote villages. Regarding the food stock, more than 1/3rd of HH surveryed did not have surplus from the last Kharif, 2/3rd of the respondents do not have seeds for the upcoming Kharif, further the study showed that63% (n= 4921) of HH is depended on the stock from the last kharif and 60% (n= 4665) of HH is depended on the stock from Rabi. Less than 20% have Kishan Credit Card among the surveyed HH. This study also shows that there has been a rapid decrease in income from livelihood activities, such is the status that there is 50% (n= 1193) reduction in milk sales and 42% (n=2875) reduction in sells of poultry. These are having a cascading effect on increased deforestation, Drudgery among women, decrease in income, possibility of school dropouts and engagement in child labour. To cope this scarcity of food, many are eating less quantity of food and lesser number of times, indicating the rapid and unavoidable malnutrition in very recent future. Further these study shows the large dependence on PDS, Food stock are depleting with time, hinting more hunger in the upcoming month and the vulnerability of HH to slip into extreme hunger. Debt has increase and so is the seed for the upcoming plantation.
This study has led us to ponder upon the situation that is going on as this study covers only few days, a week in large and tempo of pandemic is accelerating, how far the things might have evolve, situation worsened with time and what possibilities and coping mechanism is needed to combat the present scenario and what proactive approach is needed to be adopted.
To improve the nutrition among the children few best practices can be applied in any intervention areas.
1. Participatory Learning and Action: is a globally recommended community mobilization method where the member of women group invites anon-group members of the village to discuss, prioritize and strategize their health and nutritional issues prevailing in their areas. The PLA meetings are conducted by a trained local facilitator in a very structured manner. The meetings are designed in 4 phases. In the phase 1, the group identifies and prioritize their problems related to health and nutritional issues at community level. Understanding the underlying causes, the group members prepare strategies to overcome the nutritional problems in the phase 2. In the phase 3 the strategies planned will be implemented properly and act together. And in the fourth phase evaluation will be conducted to identify whether the activities planned were successfully implemented or not. This intervention is globally accepted as the recent global evidence states that integrated strategies to prevent under nutrition are more likely to succeed than discrete interventions. To maximize its benefits, the strategy includes fast acting components to address immediate determinants of under nutrition (e.g. enhanced prevention, detection and treatment for infections and improved feeding practices which includes food frequency and dietary diversity) as well as slow acting components to influence underlying determinants (e.g. Unsafe water & sanitation, women and girls empowerment).
2. Kitchen Garden: or nutritional gardens will be a sustainable model to improve the nutrition and dietary diversity of any family. The scientific way of preparation of kitchen gardens will help the family to grow fruits, vegetables and tubers in less space. Though rural areas have ample space to establish quiet a good gardens, will get sufficient vegetables and fruits required for the family, the family in urban areas could also plan for mini gardens in balconies and in terrace. Such gardens could also be planned for schools and Anganwadi centres so that the vegetable requirements for the hot cooked meal and Midday meal could be met properly. This will enhance the nutritional level among the children of the community. Studies on school gardens reveal improved nutrition and food preference in children. School gardens are known to increase consumption of fruits and vegetables, bring health and nutrition behaviour change, and have a positive effect on adolescent health. In addition, school gardens have the potential to augment physical activity and dietary intake in children. A research study from New York state schools has found potential in school gardens in improving physical activity and reducing sedentary behaviour. Along with the kitchen gardens, growing of poultry will also enhance nutrition as it gives eggs in return. The kitchen wastes could be recycled and nutritious eggs will get in return.
3. Action against Malnutrition: is an intervention to improve the nutrition of children through PLA meetings, Crèches for children between 6 months to 3 years and system strengthening. The intervention mainly focuses on community mobilisation for awareness creation and system strengthening, crèches for nutrition interventions and early childhood development. As many studies published in various international journals including The Lancet says “The effects of under-nutrition span into future generations, with a mother's nutritional status affecting the health of her future grandchildren. Conditions such as stunting, severe wasting, and IUGR in the first two years of life cause irreparable harm by impeding physical growth and—if followed by rapid weight gain in the 3–5 year age range—increasing the risk of chronic disease later in life”. So as to intervene in the nutritional need of children between 6 months to 3 years, crèches could be a good option where the children could take care of with nutritional needs. Also the crèches will support the children with early childhood care practices (ECCE).
4. Preparing nutritious food supplements: low cost food supplements could be prepared at home to meet the nutritional requirements. These food supplements could be prepared with locally available grains and nuts like millet's, wheat, Bengal gram, rice, soya beans, Jaggery, ground nuts, poha, sugar etc. These food supplements could be prepared and stored for a few months and are ready to use. Many organizations in Jharkhand promote such products prepared with local and organic products. Many women self-help groups are preparing the Nutrimix supplements, so that it will also help them to generate income by providing nutritional supplements.
- Increasing the number of anganwadi and mini anganwadi centres as per the population norms and on demand. At present the current number of AWCs in Jharkhand is 38432 and as per Census data of 2011 the total number of children was 5,389,495, It gives us the idea for the need of more AWCs as the population figures has definitely increased higher in these previous years.
- Recruitment of staff and Filling the gap of human resources in the anganwadicenters: Recruitment of qualified and trained AWW is required, some of the AWCs do not have AWW and is taken care by only AWH (Aganwadi Helpers) who are not trained in handling of AWCs.
- Capacity building of Aganwadi workers and monitoring the regular training process: to make the AWC functional and deliver the six services of ICDS schemes, the AWWs must be capacitated with update knowledge about six services, child Handling, Book keeping, ECCE and other required skills to deliver quality services. For the same community led monitoring is very important in this regard also the establishment of training centres established in different districts of the State is needed. Which would accommodate and facilitate the capacity and skill development of the AWWs and other frontline workers through trainings, workshop and seminars.
- Need crèches to cater the children between 6 months to 3 years to facilitate proper early childhood care and growth monitoring.
- Need nutritious cooked food for pregnant women and lactating mothers through Aganwadicentres along with spot feeding so that the women take nutritious food and do not hand it over to other family members, for women falling below poverty line, these cooked meal would be providing them nutrition which supplements their dietary needs which often are not available at home.
- Provision for kitchen garden for all AganwadiCentres and schools: Kitchen Garden would provide fresh, local and organic vegetables for the meals and would thus reduce the dependency on external resources. This would also help mothers and children learn the locally available food / vegetables as a source of nutrition.
- Promotion of kitchen gardens for homes: This would help the people grow organic and locally available vegetables for meeting the nutritional needs of the family, especially for the children and would further reduce their expenditure in buying vegetables from markets which are often adulterated with chemicals.
- Need at least 7 kg of grains in PDS shops. Pulses, coarse grains (Millet) and edible oils should also be provided through PDS shops: it is already stated above that provision of supplementary nutrition through PDS, MDM and AWCs are not enough to match the nutritional requirement of every individual as per the National Nutrition Institution data, and the current scenario of this pandemic period has further reduced the access, therefore, raise in quality, diversity and quantity of PDS is very crucial and needs immediate actions in this regard.
- Ration cards should be prepared immediately for the non-card holders: Pandemic has exposed and brought to light a large section of people without any identity card and Ration card and they belong to most marginalised group and falling below poverty line, which are at continuous risk of slipping into extreme hunger. It is noteworthy to mention here, that many CSOs have tirelessly worked to track these group and prepared list and submitted to various district administrations and also to various CSR funding agencies to provide these groups with basic needs of food grains and other items. These groups has to be provide with Ration card so they can have access to PDS and other services which are accessible to card holders.
- Applying a Participatory Learning and Action method to mobile the community and to create awareness among the women groups in the community: women are the change agent in the society, the success stories of SHGs groups is known to everyone. Involvement of women in dialogue regarding health and nutrition, understanding their perspective of health and Nutrition, building their perspectives in the right track and engaging them in planning, execution and monitoring of community health and Nutrition is a need of the hour. Unless ownership is develop, transparency and dialogue is promoted, ground level Health and Nutrition planning would not succeed.
- Integration of Nutrition Garden model with MGNREGS, this is already in motion and replication of this model throughout Jharkhand is important to deal with both Malnutrition and food security.
PHRN (Public Health Resource Network), EKJUT, CINI, Save the Children, Plan India, WHH, are some noteworthy expert CSOs.
A network called JASHN (Jharkhand alliance for Sustainable Health and Nutrition) was formed earlier which was later renamed as CSFCR (Civil society Network for child Rights) to address the issue of Malnutrition and was a forum of more than 80 partners NGOs.
- Rural Development Department: Integration of Nutrition Garden with the MGNREGS Schemes, which has been passed.
- PRI for development Community led monitoring of social schemes and Governance issue, Identification, discussions and involvement of Health and Nutrition issues and planning in GPDP and other community platform to pull in interest of community and make them change agents.
- Social Welfare Department: For starting discussion on THR Funding.
- Health Department : for redressal of gaps in provision of ANC( Anti Natal Care) and PNC( post natal Care) in rural areas, Provision of MCP card and other health facilities in rural areas.
- Drinking water and sanitation Department: For provision of access to safe drinking water and sanitation in Aganwadi centres, schools and for kitchen Garden as it is one of the main component of Health and Nutrition. Running water project is implement in some areas therefore replication of the same in remote areas.
- Welfare Department.
- District Mineral Fund: District having mining have District Mineral Fund, therefore these funds can be pulled for various nutrition programme and activities in areas having huge health concerns and urgencies.
- MGNREGS: for Integration of Nutrition Garden with the MGNREGS Schemes,